

Allergic Asthma: Causes, Symptoms, Diagnosis, and Treatments


Related products
Allergic Asthma Overview
Allergic asthma is a chronic respiratory condition characterised by the immune system's overreaction to specific allergens. Allergic asthma is a chronic respiratory condition that affects millions of people worldwide. It is a subtype of asthma that is triggered by exposure to allergens, resulting in inflammation and constriction of the airways. This article aims to provide a comprehensive overview of allergic asthma, including its causes, symptoms, and available treatment options.
It is essential for people with allergic asthma to comprehend the conditions, their symptoms, and the available treatment options. People with asthma effectively control their symptoms, prevent exacerbation, and generally enhance the quality of their lives by making lifestyle changes, adhering to an action plan, and collaborating with healthcare specialists. For those suffering from allergic asthma, current research in the field has the potential to lead to even more improvements.
Understanding the causes of allergic asthma is crucial for effective prevention and management strategies. A genetic predisposition, allergen sensitisation, immunological dysregulation, environmental exposures, airway hyper-responsiveness, obesity, and occupational triggers all contribute to the development and exacerbation of allergic asthma.
Allergy-related asthma is significantly influenced by genetic factors. People are more likely to develop asthma themselves if they have a family history of the disease or other allergy diseases. Numerous genes, including those involved in immunological control, airway hyper-reactivity, and lung development, have been linked to the pathophysiology of allergic asthma. Mutations in these genes influence a person's tendency for allergic responses and eventual development of asthma.
Asthma caused by allergies is frequently triggered by occupational exposure to numerous chemicals. Due to exposure to irritants or allergens like chemicals, dust, or fumes, certain professions, such as farming, woodworking, and chemical manufacture, pose a higher risk. A significant share of adult-onset asthma illnesses are caused by occupational factors. These stimuli from the workplace can cause airway hyper-responsiveness and persistent inflammation for people who are sensitive.
Asthma is characterised by recurrent episodes of wheezing, shortness of breath, chest tightness, and coughing. Coughing releases sputum from the lung, but it is challenging to remove. Due to elevated amounts of eosinophilic white blood cells, it looks pus-like while recovering after an asthma episode (exacerbation). Typically, symptoms get worse at night, in the morning, after exercise, or in cold weather.
The diagnosis of allergic asthma typically involves a combination of medical history, physical examination, and specific tests. Allergy testing helps identify specific allergens that trigger asthma symptoms. There are two main types of allergy tests: skin tests and blood tests. Skin tests involve pricking the skin with tiny amounts of allergens and observing for an allergic reaction. Blood tests measure the levels of specific antibodies (immunoglobulin E or IgE) produced in response to allergens.
The doctor occasionally conducts a challenge test to confirm the diagnosis of allergic asthma. These tests include exposing the patient to potential allergens in a safe setting while keeping an eye on the symptoms and lung function.
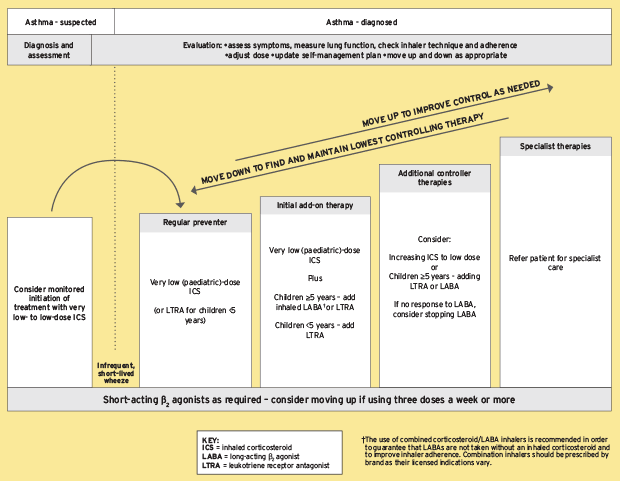
Although asthma is not cured, symptoms are usually reduced. Finding causes of asthma, such as cigarette smoke, pets, or other allergies, and avoiding exposure to them are the most effective asthma treatments. Utilising medication is advised if trigger reduction is insufficient. Pharmaceuticals are chosen, among other things, based on the severity of the sickness and how frequently the symptoms occur.
The use of bronchodilators is advised for temporary symptom reduction. No further medication is required for patients who experience sporadic attacks. Low-dose inhaled corticosteroids are advised if mild chronic illness is present (more than two attacks per week), although oral leukotriene antagonists or mast cell stabilisers are also an option. A greater dosage of inhaled corticosteroids is given to people who experience attacks on a daily basis. When an exacerbation is moderate or severe, oral corticosteroids are added to these therapies.
An essential part of controlling asthma has been highlighted as raising awareness of the condition and implementing a documented action plan. It is probably helpful to offer instructional sessions that include information particular to a person's condition. According to the World Health Organization, risk factors include tobacco smoking, air pollution, chemical irritants like perfume, and the prevalence of lower respiratory diseases must be reduced. Limiting a woman's exposure to smoking while she is pregnant, nursing and more exposure to daycare or large families are other potential initiatives, but none of these has adequate evidence to be advised for this indication.
What is allergic asthma?
Allergic asthma is a respiratory condition characterised by inflammation and breathing difficulties or tightness of the airways. Airway inflammation occurs when the mucus membrane and fluid-filled airway lining swells and constricts. Bronchospasm occurs when the muscles that surround the airways tighten and constrict in an effort to keep the airways open. Patients are left with a cough, wheezing fit, pressure in their chests and shortness of breath. Allergies and asthma are two very different disorders. But they are closely associated with one another. It's crucial to understand that not all persons with asthma also have allergies. Additionally, not everyone who has allergies also has asthma.
A hyperactive immune system is present in people with allergic disorders. Their immune systems respond to things that are generally safe. This is referred to as an allergic reaction.
It is thought that a mix of hereditary and environmental factors contribute to allergic asthma. When it comes to the onset of asthma, genetics frequently play an important influence. A family history of asthma or allergies raises the potential of developing asthma. Therefore, it's crucial to comprehend the patient's family history.
Researchers have discovered that individuals with allergic asthma are typically younger and more likely to test positive for skin allergens than those with non-allergic asthma. Allergic asthma is found most commonly in the female gender than in the male gender.
Allergy-related asthma is significantly influenced by genetic factors. People are more likely to develop asthma themselves if they have a family history of the disease or other allergy diseases. Numerous genes, including those involved in immunological control, airway hyper-reactivity, and lung development, have been linked to the pathophysiology of allergic asthma. Mutations in these genes influence a person's tendency for allergic responses and eventual development of asthma.
Sensitisation to certain allergens is one of the main factors that contribute to allergic asthma. These allergens include dust mites in the home, pollen, dander from animals, microbes from mold, and specific foods. When these allergens are exposed to those who are at risk, their immune systems generate a stronger reaction, which results in airway inflammation and bronchoconstriction. The onset and worsening of allergic asthma are both influenced by a variety of environmental factors. The symptoms of asthma are exacerbated by outdoor allergens like pollen and air pollutants including smoking, particle matter, and volatile organic compounds (VOCs). Additionally, viral respiratory infections worsen pre-existing symptoms of asthma or raise the chance of getting it, especially in young children.
It is difficult to distinguish between allergic and non-allergic asthma. This is because both types of asthma symptoms, such as coughing, wheezing, chest tightness, and shortness of breath, are the same. The main distinction is that allergic asthmatics typically exhibit symptoms after breathing an allergen. The allergic asthmatic patients develop skin rashes or other non-respiratory allergic symptoms.
A two-pronged approach is often recommended when treating allergic asthma. Both asthma and allergies need to be treated.
There are numerous allergy therapy options. Antihistamines are the initial phase for treating allergic asthma. The molecules released during allergic reactions, such as histamine, are blocked by antihistamines medications. These medications are used as needed, although depending on the allergen, they commonly work best if taken daily during allergy season.
Patients with asthma are treated with a number of drugs. Some medicines prevent or reduce inflammation of the airways. Others stop the allergic response that results in symptoms. Others ease wheezing and coughing, which facilitates breathing. Some individuals believe that asthma may be outgrown, however, this is incorrect. You don't really outgrow asthma even if your symptoms go away with time since asthma can lead to changes in the airway.
However, some people do overcome some allergies, or more specifically, their bodies don't react to certain allergens as strongly.
How does allergic asthma differ from other type of asthma?
Worldwide, millions of people suffer from chronic respiratory diseases known as asthma. It causes symptoms including coughing, wheezing, shortness of breath, and chest tightness because the airways are inflamed and narrowed. There are several different forms of asthma, but allergic asthma stands out for its particular triggers and underlying immunological reactions. With a focus on its causes, symptoms, diagnosis, and available treatments, this article seeks to analyse the unique characteristics of allergic asthma in comparison to other types of asthma.
Allergic asthma, also known as extrinsic asthma, is a subtype of asthma that is primarily triggered by allergens. These allergens include dust mites, pet dander, pollen, mold spores, and certain foods. Allergic asthma is the most common form of asthma, accounting for approximately 60-80% of all asthma cases.
The underlying immunological response is one of the main characteristics of allergic asthma. Exposure to allergens causes an overreaction of the immune system in those with allergic asthma. When the immune system determines that an allergen is dangerous, it releases substances including histamines, leukotrienes, and cytokines. Asthma symptoms are brought on by these substances, which irritate and narrow the airways.
In contrast to other types of asthma, allergic asthma is only brought on by allergens. These allergies differ from person to person, they frequently include things like pollen, pet dander, dust mites, and mold. When a person who suffers from allergic asthma is exposed to these triggers, their immune system responds and starts the inflammatory process in the airways.
The signs of allergic asthma are identical to those of other forms of asthma. They include wheezing, chest tightness, shortness of breath, coughing, and difficulty breathing. However, compared to non-allergic asthma triggers, allergic asthma symptoms typically become more severe after exposure to specific allergens.
A thorough physical examination, medical history analysis, and specialised tests are used to diagnose allergic asthma. The exact allergens that cause asthma symptoms can be determined with the aid of allergy skin testing or blood tests. These tests assess the concentrations of particular immunoglobulin E (IgE) antibodies produced in response to different allergens.
Similar to other forms of asthma, allergic asthma is treated by focusing on symptom management and avoiding asthma attacks. Long-term controller drugs, such as inhaled corticosteroids, leukotriene modifiers, and long-acting beta-agonists, are frequently used with short-acting emergency inhalers to provide instant relief during asthma attacks. Additionally, it may be advised to take allergen prevention measures including utilising mattress coverings, routine cleaning, and excluding dogs from the bedroom. Allergen immunotherapy, sometimes referred to as allergy shots, is one distinctive method of treating allergic asthma. In order to desensitise the immune system over time, this treatment includes exposing the patient to steadily increasing dosages of the allergen. In some people with allergic asthma, allergen immunotherapy help to lessen symptoms and the need for medication.
A severe asthma attack and potentially fatal consequences result from allergic asthma if it is not properly managed. Working closely with their healthcare professionals, people with allergic asthma must create an asthma action plan that addresses effective medication management, regular check-ups, and recognising and avoiding triggers.
Is allergic asthma common?
Yes, In certain demographics and geographical areas, allergic asthma is more prevalent than other types of asthma. According to the Global Asthma Report 2018, there are 300 million asthma sufferers globally, with allergic asthma being the most common type. According to studies, many cases of asthma are allergic in origin in industrialised nations like the United States and Europe, Up to 90% of asthma cases in children and 50% to 70% of cases in adults have been found to have allergic sensitisation.
In recent years, allergic asthma has become more common, especially among youngsters and in urban environments. Numerous causes, such as increasing exposure to environmental allergens, dietary and lifestyle changes, and decreased microbial diversity, are responsible for this increase. Furthermore, as those who have a family history of allergies or asthma are more likely to develop allergic asthma, genetic predisposition also contributes to the condition.
For those who suffer from allergic asthma, their quality of life is significantly impacted. It is linked to repeated symptoms, restrictions on physical activity, sleep problems, and a higher risk of asthmatic recurrence Chronic airway inflammation increases the risk of developing various respiratory disorders, including chronic obstructive pulmonary disease (COPD), as well as long-term lung damage and decreased lung function. Additionally, allergic asthma, especially in children and adolescents, has a significant psychological and emotional impact, including anxiety, despair, and social isolation.
Additionally, allergic asthma has a significant financial impact on both patients and healthcare systems. Medication costs, doctor appointments, visits to the ER, and hospital stays are examples of direct costs. As a result of missing work or school days and lower work productivity, indirect costs occur. Costs associated with asthma surpass $80 billion yearly in the US alone.
Strategies for managing allergic asthma include reducing exposure to triggers, maintaining symptom control, and avoiding recurrence Utilising bedding that is allergy-proof, getting rid of carpets, and maintaining regular cleaning will assist limit allergen exposure at home. Leukotriene modifiers, long-acting beta-agonists, inhaled corticosteroids, and immunomodulators are a few examples of pharmaceutical therapies. These drugs aid in reducing inflammation, easing airway tension, and enhancing lung capacity.
It has been demonstrated that immunotherapy, in particular subcutaneous or sublingual allergen immunotherapy, is beneficial in easing allergic symptoms and altering the course of the disease. In order to gradually desensitise the immune system, this treatment includes giving patients progressively higher dosages of allergens.
Programs for self-management and education are essential for helping people with allergic asthma understand and control their condition. Important elements of self-management for asthma include asthma action plans, routine symptom monitoring, peak flow measurements, and appropriate use of rescue drugs. Additionally, creating a supportive atmosphere at school and work where asthma triggers are kept to a minimum greatly enhances the well-being of people who suffer from allergic asthma.
What are the causes of allergic asthma?
Understanding the causes of allergic asthma is crucial for effective prevention and management strategies. A genetic predisposition, allergen sensitisation, immunological dysregulation, environmental exposures, airway hyper-responsiveness, obesity, and occupational triggers all contribute to the development and exacerbation of allergic asthma.
Allergy-related asthma is significantly influenced by genetic factors. People are more likely to develop asthma themselves if they have a family history of the disease or other allergy diseases. Numerous genes, including those involved in immunological control, airway hyper-reactivity, and lung development, have been linked to the pathophysiology of allergic asthma. Mutations in these genes influence a person's tendency for allergic responses and eventual development of asthma.
Asthma caused by allergies is frequently triggered by occupational exposure to numerous chemicals. Due to exposure to irritants or allergens like chemicals, dust, or fumes, certain professions, such as farming, woodworking, and chemical manufacture, pose a higher risk. A significant share of adult-onset asthma illnesses are caused by occupational factors. These stimuli from the workplace can cause airway hyper-responsiveness and persistent inflammation for people who are sensitive.
Listed below are some causes of allergic asthma:
1. Pollen
Pollen plays a significant role in allergic asthma, which is a type of asthma triggered by exposure to specific allergens. When exposed to allergens, the airways swell and narrow, causing symptoms including chest tightness, coughing, wheezing, and shortness of breath. In those who are vulnerable, pollen, a frequent allergen of the air, can cause or aggravate the symptoms of allergic asthma.
Pollen is a common allergen that is released by plants, especially trees, grasses, and weeds, during their reproductive cycle. Due to their small size and ease of airborne dispersion, these tiny particles easily cross large distances and reach the respiratory system.
People who have allergic asthma will experience an immunological reaction when they breathe in pollen particles because their immune system interprets the pollen. In reaction to exposure to pollen, the immune system creates particular antibodies termed immunoglobulin E (IgE). These antibodies attach to mast cells, which are found in various organs like the airways.
Following a second encounter with pollen, the mast cells' related IgE antibodies identify the allergen and cause the production of several substances, including histamine. Histamine and other mediators in the airways trigger immunological reactions such as inflammation, bronchoconstriction (narrowing of the airways), and increased mucus production.
The severity of allergic asthma symptoms varies depending on the individual's sensibility to pollen, the amount of pollen exposure, and other factors. Pollen levels in the environment tend to be higher during certain seasons, such as spring and fall when plants release their pollen. Therefore, individuals with allergic asthma often experience seasonal exacerbations of their symptoms, commonly known as seasonal allergic asthma.
2. Dust Mites
Dust mites are tiny, insect-like pests that live in warm, humid environments and feed on the dead skin cells of humans. People don't detect dust mites because they are too little. They aren't parasites that irritate the skin bites or bury themselves in our bodies. People who are allergic to dust or dust mites, actually react when they breathe in dust particles that include proteins from dead bodies, urine, or faeces of dust mites. dust mites cause nasal swelling and dust allergy.
In almost every home, dust mites are found naturally. The most crucial element in assessing whether a home has a high amount of dust mites is humidity. This is because those mites take moisture from the air as dust mites do not drink water like humans do. Dust mites are unable to flourish in dry environments like deserts.
Dust mite allergens often don't remain in the air, in contrast to pet allergens. Instead, the allergen readily binds to dust or fibres. Mites allergens stick to carpets, sleepwear, pillows, sofas and chairs, drapes, and other surfaces that act as colonies. The majority of dust mite allergy contact happens during sleep.
For people who have asthma, dust mites are one of the main indoor triggers. People with asthma, those who are allergic to or sensitive to mites, and those who live in homes where dust mites are present experience health effects. Asthma episodes result from exposure to mites allergens, which cause mild to severe allergy symptoms. Watery eyes, a runny nose, and the occasional sneeze are possible symptoms of mild allergic asthma. In severe situations, the problem persists and causes ongoing sneezing, coughing, congestion, pressure on the face, or even a severe asthma attack. Asthma episodes are more likely to occur in people with asthma who are allergic to dust mites.
The pathophysiology of dust mite allergy involves IgE-mediated sensitisation. This hypersensitive reaction is a type 1 hypersensitivity reaction in which the CD4 + and T helper cells stimulate the B cells to make IgE antibodies specific to the antigen, which is the house dust mite allergen. Mast cells and blood basophil cells have FceRI receptors that the IgE binds to. Now, the allergen-specific IgE antibodies sensitise the mast cells and basophil cells. The bound IgE-sensitised cells crosslink when exposed to the same allergens again, which causes their breakdown. The clinical manifestation of the dust mite allergy is brought on by the release of inflammatory markers. Early-life sensitisation to dust mite allergens result in a transition from allergic to allergic asthma.
4. Mold Spores
A mold is a form of fungus that releases spores into the atmosphere. When there is humidity or a moist atmosphere, Mold grows on nearly anything. molds are found both inside and outside. mold causes allergic and consequently allergic asthma symptoms.
An allergic reaction to mold occurs immediately. However, it sometimes results in symptoms that appear later. Asthma symptoms worsen over time as a result of this, including stuffy nose. People have a mold allergy if their symptoms frequently worsen in a moist, muggy, or moldy environment, such as a basement.
In the summer and autumn, outdoor molds frequently trigger allergy symptoms. But in hotter, more humid climes, the allergic reaction occurs throughout the year. Year-round allergy problems are brought on by indoor molds.
Occasionally, a condition known as allergic bronchopulmonary aspergillosis affects some people. In this situation, the mold or fungus causes an allergic reaction as well as an inflammatory (swelling) response in the lungs. Similar to asthma symptoms, there are significant wheezing, coughing, chest tightness, and shortness of breath.
Food fungi, such as those found in dried fruit, soy sauce, vinegar, and meals like mushrooms, rarely induce nasal, ocular, or respiratory allergic symptoms. Food's direct impact on blood vessels is a common reason for reactions to food fungus.
A natural chemical called histamine, for instance, is present in fermented foods (like wine). When patients have an allergic reaction, the allergy cells release histamine. The histamine reacts to foods and triggers allergic reactions.
4. Animal Dander
An important factor in allergic asthma is animal dander. Animal danders are microscopic fragments of skin, hair, fur, or feathers that are expelled by animals like cats, dogs, rodents, and birds. When these allergenic particles are breathed, those who are allergic to them may experience allergic reactions.
People who are exposed to animal dander may experience sensitisation, a condition in which their immune systems are abnormally sensitive to the allergens in the dander. The immune system produces certain antibodies, known as immunoglobulin E (IgE) antibodies, against animal allergens resulting in sensitisation. This sensitivity develops after the result of prolonged exposure to animal danders.
Individuals who are sensitive to animal dander experience an allergic reaction when they come into touch with it. Specific IgE antibodies bind to the allergens in pet dander, activating mast cells, which are immunological cells. Histamine is one of the chemical molecules that mast cells release that causes inflammation and airway constriction. Asthma symptoms like coughing, wheezing, chest tightness, and shortness of breath are brought on by these reactions.
Animal allergens are transferred to different surfaces, including furniture, carpets, and clothing. This cross-contamination leads to exposure even in environments where animals are not present, as allergens are carried on these surfaces and become airborne when disturbed, triggering asthma symptoms.
Minimising exposure and avoiding touch are the best ways to treat a pet allergy. When being around the animal is inevitable, people avoid animal dander from sticking by making sure that all furniture, carpets, and clothing are cleaned right away and frequently after contact. When a person came into contact with the animal directly, wash hands or even take a bath. To reduce the amount of allergens in the air, one must designate an area as a pet-free zone and utilise air cleaners.
5. Cockroach Droppings
The most common chronic disease in children is asthma, which is a growing clinical and public health problem. From 7.3% in 2001 to 8.4% in 2010, the prevalence of asthma in the United States has increased. Over 300 million individuals worldwide suffer from asthma, which is responsible for one fatality out of every 250. The cause of this rising occurrence is still not fully known, though.
It has become clear that interactions between certain genetic variables and early-life environmental factors play a significant role in the development of asthma. Cockroach antigens are widespread, and it has been demonstrated that exposure and sensitisation enhance the morbidity of asthma. Particularly among inner-city children with asthma, exposure to cockroach allergens seems to have a bigger impact on asthma morbidity than dust mites or pet allergies.
According to the Asthma and Allergy Study (NAAS), houses in areas with higher asthma prevalence have more cockroach allergens in their bed dust than those in areas with lower asthma prevalence.
Cockroach crude extract is used to identify cockroach allergy through skin testing and/or the determination of specific IgE to cockroach allergens. It has been demonstrated that cockroach allergen-specific IgE levels are connected with allergen exposure in individuals who have developed sensitisation as well as a variety of inflammatory, physiologic, and clinical signs.
Like many other indoor/outdoor allergens (such as house dust mites, fungi, pollen, and animal dander), cockroach excrement particles can enter the lungs by settling across the nasal or oral cavities, where they can cause allergic-type inflammation by allergen-induced epithelial damage or through direct contact with epithelial cells.
In addition to directly activating epithelial cells, cockroach allergens can also cause their release of cytokines and chemokines (such as TSLP, IL25, IL33, and TGF-1), which attract inflammatory cells to the allergen-damaged airway for healing and inflammation reduction.
Are there certain foods or food additives that can cause allergic asthma?
Yes, Some asthmatics patients also have food allergies. Nevertheless, even though the symptoms of food allergies resemble an asthma attack, however, food allergies occasionally cause asthma attacks. The body's allergic reaction to food is called anaphylaxis reaction. The anaphylaxis reaction cause the same symptoms as asthma, such as wheezing, coughing, and shortness of breath. Additionally, anaphylaxis results in anxiety, stomach issues, circulation issues, watery or itchy eyes, and eczema of the skin. In more severe anaphylaxis reactions death is also possible.
Any food has the potential to cause an allergic reaction in a person. However, common foods to which people have allergies include nuts, eggs, wheat, milk, shellfish, and soy. Food allergies are quite uncommon and result in indigestion.
In fact, sulfites, a common food ingredient, trigger an asthma attack or asthma symptoms, especially in persons with severe, long-lasting asthma. In contrast to allergy reactions, which involve the IgE (immunoglobulin) antibody, medical researchers do not know how sulfite produces asthma symptoms. Processed potatoes, prawns, dried fruit, beer and wine all have sulfite compounds. The main foods that contain sulfites, which trigger asthma symptoms, are wine and beer. Monosodium glutamate (MSG), yeast, and other dietary additives also aggravate asthma symptoms.
Salicylates are responsible for allergic reactions. Salicylates are a naturally occurring substance found in tomato paste, honey, beer, and coffee but are not added to food. Aspirin is a salicylate, and approximately 10% of asthmatics patients are susceptible to it.
The majority of people aren't facing allergic reactions or getting symptoms of asthma from dietary additives. Understanding food ingredients and validating others' experiences is crucial because only a small percentage of people actually experience allergic reactions. Food chemicals and additives are not identified as allergens on food packaging, except sulfite, but one can still find them in the ingredient list. Be sure to discuss this food ingredient with the doctor if you think a meal you don't recognise is responsible for your asthma or an allergic reaction.
How can cigarette smoke or air pollution cause allergic allergens?
Air pollution and cigarette smoke are two common environmental elements that harm people's health. Although their link to respiratory and cardiovascular illnesses is well known, recent research indicates that they act as allergens, causing allergic reactions in those who are sensitive.
Air pollution and cigarette smoke are now recognised as important environmental factors that influence the onset and severity of allergy reactions. It is crucial to reduce exposure to these dangerous compounds because of their capacity to interfere with immunological function, cause inflammation, and make it easier for allergens to enter the respiratory system. People lessen the influence of cigarette smoke and air pollution on allergic allergens and enhance the general well-being of those who are prone to allergies by establishing efficient public health policies, increasing knowledge, and adopting measures to avoid them.
Cigarette smoke contains numerous harmful substances, including nicotine, carbon monoxide, and volatile organic compounds (VOCs). According to research, these ingredients contain immunomodulatory properties that raise the chance of allergic sensitisation. According to studies, exposure to cigarette smoke might increase the development of IgE antibodies, making people more prone to allergic reactions. Furthermore, regulatory T cells, which are essential for preserving immunological tolerance and avoiding allergies, work less effectively in the presence of nicotine.
Air pollution is a complex mixture of particulate matter (PM), gases, and various toxic substances emitted from vehicles, industries, and natural sources. Particulate matter, especially PM2.5 and ultrafine particles, has been linked to allergy sensitisation and the aggravated of pre-existing allergies. These spores make it easier for allergens to enter the respiratory system by carrying things like pollen and fungal spores. They start immunological reactions after being breathed, causing the synthesis of IgE and the release of pro-inflammatory cytokines.
There are numerous ways that air pollution and cigarette smoke cause allergic sensitivity. First, they cause oxidative stress and inflammation in the airways, impairing the respiratory epithelium's integrity. Allergens are able to interact with immune cells when the barrier function is disrupted, allowing them to enter deeper tissues. Second, the innate immune system is activated by both cigarette smoke and air pollution, which encourages a Th2-biased immune response. This shift towards Th2 immune polarisation favours IgE production and the development of allergic reactions.
Several steps must be taken to lower the risk of allergic reactions brought on by cigarette smoke and air pollution. First and foremost, regulations and programs to help people quit smoking are crucial to preventing exposure to cigarette smoke. In addition, encouraging the use of cleaner energy and enacting stronger limits on industrial source emissions help in lowering air pollution levels. indoor air quality is improved by using air filtration devices, sufficient ventilation, and fewer VOC-emitting household goods.
What are symptoms of allergic asthma?
Recognising the symptoms of allergic asthma is crucial for early diagnosis, effective treatment, and improved long-term outcomes. Listed below are some common symptoms of allergic asthma.
Some allergic asthma sufferers have gastrointestinal problems, such as reflux, bloating, and pain in the abdomen. Certain triggers, such as stress, particular drugs, or underlying illnesses like gastroesophageal reflux disease (GERD), cause these symptoms to become apparent. However, in order to assess the particular symptoms and identify the underlying cause, it is important that you speak with a healthcare practitioner.
It's important to consult a doctor if a person has severe or persistent abdominal discomfort in order to get a proper diagnosis and treatment. A medical expert will be able to evaluate the symptoms, carry out any necessary tests, and offer specific recommendations based on the particular conditions.
1. Anxiety
Anxiety and allergic asthma commonly interact, resulting in a complex interaction between physical and mental health. In those with allergic asthma, allergens cause an immunological response that sets off a chain of events that increase stress levels and anxiety. The persistent worry of having an asthma attack and the associated restrictions on everyday activities brought on by allergic asthma have a serious negative effect on a person's mental health. Anxiety makes allergic asthma symptoms worse by causing hyperventilation and bronchoconstriction.
In people with allergic asthma, a number of variables lead to an increase or worsening of anxiety. First, the irregular characteristics of asthma episodes and the corresponding fear of suffocation cause a lot of anxiety. The mental pain brought on by the perception of a threat to one's own or a loved one's life starts a cycle of worry and anxiety. In addition, the restrictions put in place by allergic asthma, such as avoiding specific places or activities, cause social isolation, low self-esteem, and heightened anxiety.
Additionally, the brain and neurotransmitter systems are directly impacted by the chronic inflammation and immunological dysregulation associated with allergic asthma. According to studies, pro-inflammatory cytokines that are generated during allergic reactions affect the neurotransmitter systems that control mood, making anxiety feelings more likely. Furthermore, as corticosteroids have psychological adverse effects, their usage in the treatment of asthma potentially increases anxiety.
2. Fatigue
Fatigue is a common symptom of people with allergic asthma, Although it is usually masked by the more noticeable respiratory symptoms. A number of factors play a role in its emergence, Although the exact mechanisms causing fatigue associated with allergic asthma are not fully known.
Due to nocturnal symptoms of allergic asthma, such as coughing and breathing difficulties, sleep patterns are disturbed. These disruptions cause poor sleep, which causes exhaustion during the day and low energy levels.
Asthma attacks cause the airways to constrict, which makes breathing difficult. This results in less oxygen intake, which would deprive the body's tissues and organs of oxygen. Lack of oxygen cause fatigue because it is necessary for the generation of energy. Various molecules and cytokines are released as a result of an immunological reaction brought on by the chronic inflammation linked to allergic asthma. These chemicals have the ability to spread symptoms of malaise and tiredness throughout the body.
An individual's quality of life is greatly impacted by fatigue in allergic asthma. Constant fatigue makes it difficult to exercise and engage in physical activity, which limits engagement in social and daily activities. Additionally, it disrupts cognitive function, impairing focus, memory, and general productivity. In addition, a cycle of physical and mental tiredness is created by the presence of respiratory problems and fatigue, which lower motivation and raise stress levels.
3. Coughing
A chronic cough is another common sign of allergic asthma. This cough is dry or accompanied by mucus production. It is brought on by allergens or physical exercise and seems to happen more frequently at night or in the early morning. Additionally, respiratory illnesses and exposure to irritants like smoke or potent smells make the cough worse.
4. Shortness of Breath
People who have allergic asthma could feel short of breath or have breathing problems. Depending on the patient and the occurrence of triggers, the severity of this symptom ranges from minor to severe. The influence of shortness of breath on physical activity and exercise tolerance is considerable. It is sometimes accompanied by tightness in the chest.
5. Wheezing
Wheezing is one of the most noticeable symptoms of allergic asthma. Wheezing is the term used to describe a high-pitched whistling sound that happens when breathing. Due to inflammation and excessive mucus production, it is brought on by airway constriction. Wheezing occurs both during inhalation and exhalation, however, it is more obvious during the exhalation. When exposed to allergens or triggers like dust mites, pollen, pet hair, or specific foods, people with allergic asthma frequently report that their wheezing gets worse.
6. Chest Tightness
Chest tightness, which is characterised by a feeling of pressure or constriction in the chest area, is frequently brought on by allergic asthma. It is challenging to take deep breaths since it seems like a heavy weight is weighing downward toward the chest. Chest tightness is often caused by exposure to allergens or other asthma triggers, and it frequently coexists with other symptoms including wheezing and shortness of breath.
7. Difficulty Breathing
Among the various symptoms experienced by individuals with allergic asthma, breathing difficulty stands out as one of the most distressing and debilitating. A distinctive sign of allergic asthma is difficulty breathing. It happens as a result of the airways' inflammation and narrowing, which prevents enough air from getting into and out of the lungs. An allergic asthmatic person's immune system overreacts to certain allergens, which causes an inflammatory response in the airways. This inflammation causes swelling, an increase in mucus production, and bronchoconstriction, or the tightening of the muscles that surround the airways.
Breathing problems are significantly exacerbated by bronchoconstriction. Shortness of breath and the distinctive wheezing sound are caused by the constrictions in the airways, which make it more difficult for air to pass through. Breathing problems range in intensity from minor to severe, and can sometimes turn life-threatening, requiring emergency medical attention.
The quality of life of a person with allergic asthma is greatly impacted by breathing difficulties. For those with allergic asthma, simple actions like walking up stairs, working out, or even talking can become challenging. The persistent effort to breathe causes exhaustion, worry, and a decrease in physical activity.
8. Rapid Breathing
Rapid breathing, also known as tachypnea, is one of the many symptoms experienced by people with allergic asthma and is a major cause for concern.
In allergic asthma, being exposed to allergens like pollen, dust mites, or pet dander causes an immunological reaction that inflames the airways. Due to the swelling and constriction of the airway walls brought on by this inflammation, it is more difficult for air to freely enter and exit the lungs. Rapid breathing results from the body's response to speeding up breathing.
In allergic asthma, rapid breathing causes hyperventilation, a condition marked by an imbalance in oxygen intake and carbon dioxide output. This results in a feeling of lightheadedness, dizziness, and tingling in the extremities. Hyperventilation worsens respiratory distress and, in certain people, brings on panic attacks.
Additional symptoms include the following:
Allergic Rhinitis Symptoms
The symptoms of allergic rhinitis, or hay fever, are frequently present in people with allergic asthma. Sneezing, watery or itchy eyes, a runny or clogged nose, and an itchy or scratchy throat are some of these symptoms. The combination of allergic rhinitis and allergic asthma is frequently referred to as "allergic rhinoconjunctivitis" and aggravate respiratory symptoms.
Skin rash
Both allergic asthma and skin rashes are prevalent illnesses that have a major influence on a person's quality of life. Despite the fact that allergic asthma mostly affects the respiratory system, research indicates a possible connection between allergic asthma and skin rashes.
Research points to a possible connection between allergic asthma and skin rash. There are many potential contributing reasons to this association, even though the precise underlying mechanisms are still unknown. The common allergic reaction in the skin and respiratory systems is one theory that has been put forth. The immune system is frequently overactive in people with allergic asthma, increasing their sensitivity to and responsiveness to different allergens. Rashes on the skin are one possible manifestation of this immunological dysregulation.
Another theory is based on the systemic inflammatory response to allergic asthma. Studies have demonstrated that persistent respiratory system inflammation leads to inflammatory reactions in the skin and other bodily tissues. This causes skin rashes to appear as an outward sign of the underlying inflammation.
How does the symptoms of allergic asthma differ in adults and children?
All ages are affected by allergic asthma, but there are differences between adults and children in terms of signs and clinical manifestations. For appropriate management and therapy, it's essential to comprehend these differences.
Allergic asthma is a common respiratory condition that affects people of all ages, with a high prevalence in both children and adults. However, studies show that childhood onset is more common, with a considerable portion of affected individuals continuing to exhibit symptoms throughout adulthood. Allergic asthma in children frequently begins before the age of six, while adult-onset allergic asthma normally begins after the age of 20.
Compared to children, adults with allergic asthma typically experience more severe and long-lasting symptoms. They often cough, particularly at night or in the morning. Adult patients frequently experience chest tightness, wheezing, and shortness of breath. These symptoms are frequently brought on by exposure to allergens such as dust mites, pollen, pet dander, or particular foods. When under stress or as a result of respiratory illnesses, these symptoms could get worse.
Children with allergic asthma may experience sporadic and episodic symptoms. The most common symptom is coughing, especially after exercising or after being exposed to certain triggers. In children with asthma, wheezing—a high-pitched whistling sound made during exhalation—is frequently heard. Chest constriction, rapid breathing, and trouble engaging in physical activity are possible in younger children. Allergens, respiratory illnesses, exertion, or exposure to tobacco smoke all cause symptoms.
Adult allergic asthma is frequently accompanied by sensitization to a wider variety of allergens, such as dust mites, pollen, mold spores, animal dander, and some occupational allergens. The treatment and avoidance of certain allergens are crucial for symptom control because sensitivity to them results in more severe and enduring symptoms.
The most frequent causes of allergic asthma in children are often pollen, animal dander, and house dust mites. The symptoms of certain allergies worsen or flare up when someone is sensitive to this allergen. Additionally, food allergens like peanuts or shellfish, which cause allergic responses and asthma symptoms, are more likely to affect children than adults.
Adults who have allergic asthma commonly also experience rhinitis (hay fever) and sinusitis. These illnesses' nasal symptoms, such as nasal congestion, sneezing, and a runny or itchy nose, make asthma symptoms worse. Additionally, chronic respiratory conditions such as chronic obstructive pulmonary disease (COPD) or bronchiectasis coexist with allergic asthma, resulting in worse symptoms and decreased lung function.
In children, allergic asthma frequently coexists with other allergy diseases such as allergic rhinitis and atopic dermatitis (eczema). These diseases raise the likelihood of acquiring asthma. To manage children's asthma symptoms properly, it's crucial to address these comorbidities.
Inhaled corticosteroids (ICS) are frequently used as a first-line therapy to reduce airway inflammation in the pharmacological management of allergic asthma in adults. As a supplement to therapy, leukotriene modifiers or long-acting beta-agonists (LABA) are administered. Biologic treatments that target specific immune pathways are considered in extreme situations. Adult asthma management includes important lifestyle changes like quitting smoking and avoiding allergens.
A similar pharmaceutical strategy is used to treat allergic asthma in children as it is in adults. Inhaled corticosteroids (ICS) are frequently recommended to treat symptoms and reduce inflammation. During acute episodes, short-acting beta-agonists (SABA) offer relief. The management of symptoms in children is greatly aided by asthma action plans and education for parents and other caregivers. Long-term control requires identifying and avoiding triggers, keeping excellent indoor air quality, and implementing effective allergy management.
How does Allergic asthma diagnose?
A thorough process is used to diagnose allergic asthma, including a thorough review of the patient's medical history, symptom evaluation, physical examination, lung function tests, allergy testing, and, if necessary, challenge tests. Accurate diagnosis enables medical professionals to create specific treatment plans that include methods for avoiding allergens, medications, and patient education, improving management and quality of life for people with allergic asthma.
The first step in diagnosing allergic asthma involves obtaining a detailed medical history and conducting a thorough symptom assessment. The medical professional will ask the patient about their symptoms, such as coughing, wheezing, shortness of breath, and pressure in their chest. They will look into things like exercise, cold air, respiratory illnesses, and exposure to allergens as possible causes or aggravating issues. The doctor will evaluate the patient's daily routine and sleeping habits as well as the frequency, duration, and severity of their symptoms.
After going through the patient's medical history, a physical examination is carried out to look for any asthmatic symptoms or signs. The medical professional will use a stethoscope to listen to the patient's lungs and listen for any abnormal respiratory findings, such as wheezing or diminished breath sounds. In addition to checking the nasal passages, they look for allergic diseases like eczema or rhinitis, which generally coincide with allergic asthma.
The diagnosis of allergic asthma depends heavily on the results of lung function testing. These examinations measure the efficiency with which the lungs can inhale and exhale air as well as how well the airways are working. The two most common tests used are the spirometry and Peak Expiratory Flow (PEF) test.
Spirometry assesses how much air a person can forcibly exhale after taking a deep breath. It helps in evaluating lung performance, including airflow and volume. An obstructive pattern, a recognisable pattern that indicates airway blockage in allergic asthma, is able to be seen with the help of spirometry.
In PEF monitoring, the fastest rate at which a person forcibly exhales air is measured using a handheld device called a peak flow meter. Regular PEF monitoring aid in detecting fluctuations in airflow and determining the severity of asthma symptoms.
Effective management of allergic asthma depends on recognising the specific allergens that cause it. For the purpose of identifying the presence of allergen-specific antibodies, allergy testing is carried out via skin prick tests or blood tests (specific IgE). Small amounts of allergens are applied to the skin's surface during skin prick testing, and an allergic reaction is subsequently monitored immediately. Antibodies that are specific to allergens are determined during blood tests. These tests support the creation of specific treatment regimens by identifying the allergens to which a person is hypersensitive.
In order to determine the diagnosis of allergic asthma, challenge tests are sometimes necessary. These investigations involve carefully monitoring the patient's symptoms and lung function while exposing them to suspected allergens or triggers under controlled circumstances. In order to make a proper diagnosis, medical professionals rule out further possible causes of respiratory symptoms, such as chronic obstructive pulmonary disease (COPD), vocal cord dysfunction, or cardiac issues.
What are the treatment and medications for allergic asthma?
An all-encompassing strategy that involves precautions, medication, and preventive therapies is required for the management of allergic asthma. Reducing triggers and preventing asthma episodes depend heavily on patient education, allergen avoidance, and environmental management. In order to alleviate symptoms and enhance lung function, doctors frequently prescribe drugs including inhaled corticosteroids, long-acting beta-agonists, leukotriene modifiers, and short-acting beta-agonists. Immunomodulators and combination inhalers could be required for people with severe allergic asthma.
Exciting new medicines have the potential to advance the field of therapy and enhance outcomes for people with allergic asthma. Examples include bronchial thermoplasty and biological agents. In order to create a customized treatment plan that efficiently manages their symptoms and improves their quality of life, patients must collaborate closely with medical specialists.
Avoiding triggers is the first line of protection for treating allergic asthma. People ought to identify their unique allergens and take precautions to reduce exposure. This includes avoiding environmental triggers like pollen and pollution as well as maintaining clean, mold- and dust-mite-free, pet-free inside surroundings.
Putting environmental controls in place might lessen exposure to allergens further. This entails the use of high-efficiency particulate air (HEPA) filters, the use of allergen-resistant covers for mattresses and pillows, frequent hot water bed washings, and the maintenance of low humidity levels.
1. Inhaled Corticosteroids
Inhaled corticosteroids(ICS) are the most effective medications for allergic asthma. Inhaled corticosteroids primarily do this function by recruiting the enzyme histone deacetylase 2 (HDAC2) to reverse histone acetylation, which turns off a number of active inflammatory genes.
With the help of reducing inflammatory airway response, ICS alleviate asthma symptoms and lessen airway hyperresponsiveness. ICS are now the first-line treatment option for managing asthma symptoms and avoiding exacerbations for all patients with chronic asthma. Inhaled long-acting 2-agonists are frequently administered in addition to ICS to further improve asthma control, which increases compliance and manages asthma at lower dosages of corticosteroids, In COPD, however, ICS offer substantially less therapeutic benefit, because the inflammation is resistant to corticosteroid impact.
At the cellular level, inhaled corticosteroids diminish the amount of inflammatory cells, such as eosinophils, T lymphocytes, mast cells, and dendritic cells, in asthmatic airways. These effects of corticosteroids are brought about by reducing the creation of chemotactic mediators and adhesion molecules as well as by preventing inflammatory cells like eosinophils, T-lymphocytes, and mast cells from surviving in the airways.
As corticosteroids and inhaled beta 2-agonists are routinely used in conjunction to treat asthma, it is now understood that these two groups of medications have significant molecular interactions. The expression of cell surface receptors is raised by corticosteroids due to a rise in the gene transcription of beta 2 receptors.
Due to their poor response to corticosteroids, people with severe asthma require high dosages of the medication, and a small number of them develop total resistance. The majority of COPD patients exhibit corticosteroid resistance. Smokers with asthma are generally more corticosteroid resistant and need higher corticosteroid dosages to control their asthma.
2. Immunomodulators
Numerous different cells, mediators, and cytokines are involved in the pathophysiology of asthma. It is also clear that certain molecules or pathways have a bigger role in some patients than others. Therefore, it is difficult to find a universal therapy that would be clinically advantageous for all individuals.
Immunomodulators play an important role in the management of allergic asthma. Immunomodulators are drugs that assist in controlling and modifying the immune system's reaction. Immunomodulators are used to control the heightened immune reaction to allergens in the setting of allergic asthma, thereby lowering inflammation and airway hyperresponsiveness.
Monoclonal antibodies are a more recent family of immunomodulators that target particular immune response-related components. Omalizumab and dupilumab are examples of monoclonal antibodies that are used to treat allergic asthma. Immunoglobulin E (IgE), a factor in allergic reactions, is inhibited by omalizumab. Dupilumab targets interleukin-4 (IL-4) and interleukin-13 (IL-13), which are involved in the allergic inflammatory response.
Depending on how severe the asthma is and how the patient responds to treatment, these immunomodulators are used singly or in combination. They need regular modifications and are often given by healthcare professionals based on the particular requirements of the patient.
It is significant to remember that the use of immunomodulators must be overseen by a medical expert skilled in treating allergic asthma. They determine the extent of asthma, assess the advantages and potential drawbacks of each medicine, and modify the treatment strategy as necessary.
3. Leukotriene Modifiers
Leukotriene modifiers are a family of drugs used to treat allergic asthma. They function by focusing on leukotrienes, which the body's immune cells release in response to an allergic reaction. Leukotrienes produce inflammation, bronchoconstriction (narrowing of the airways), and mucus formation in the lungs, which result in asthma symptoms.
There are two types of leukotriene modifiers commonly used in the treatment of allergic asthma: leukotriene receptor antagonists (LTRAs) and 5-lipoxygenase inhibitors.
Leukotriene Receptor Antagonists (LTRAs): These drugs bind to the receptors where leukotrienes would typically attach, blocking the effect of leukotrienes. LTRAs do this by preventing the development of mucus, inflammation, and smooth muscle contraction brought on by leukotrienes in the airways. Examples of LTRAs include montelukast, zafirlukast, and pranlukast.
5-Lipoxygenase Inhibitors: These drugs block the action of the leukotriene-producing enzyme 5-lipoxygenase. 5-lipoxygenase inhibitors work by inhibiting this enzyme, which lowers the entire generation of leukotrienes and lowers inflammation and asthma symptoms.
Leukotriene modifiers are frequently used in conjunction with inhaled corticosteroids (ICS). They are especially helpful for people with allergic asthma whose symptoms are difficult to manage with ICS alone. Leukotriene modifiers aid in bettering asthma management, lowering the frequency and intensity of asthma attacks, and lowering the requirement for emergency drugs.
4. Combination Inhalers
The long-term management of asthma symptoms is managed with the help of combination asthma inhalers. They mix a corticosteroid and a long-acting beta-agonist (LABA), which are two separate inhaled drugs. LABAs are bronchodilators that widen and open congested airways to allow for the free flow of air, whereas corticosteroids reduce inflammation. These drugs work better together to reduce airway hyperresponsiveness and prevent asthma attacks.
LABA functions by relaxing the smooth muscles that surround the airways, which opens up the airways and enhances airflow. Wheezing and breathlessness are reduced as a result of this. Formoterol and salmeterol are two commonly used LABAs.
The combination inhaler's ICS ingredient aids in lowering airway inflammation, which is a significant contributor to allergic asthma. In order to reduce swelling and mucus production, it works by inhibiting the inflammatory reaction in the airways. ICSs enhance overall asthma management by reducing inflammation, which helps to prevent asthma episodes. Fluticasone, budesonide, and beclomethasone are ICSs that are often utilised.
Combination inhalers make managing asthma easier by minimising the number of inhalers a patient needs to use. This convenience improves medication compliance and lowers the possibility of the administration of medication problems.
Compared to utilising a LABA or an ICS alone, combination treatment offers more effective management of asthma symptoms. It successfully treats the underlying inflammation as well as the signs and symptoms of bronchoconstriction, which results in better asthma control and a lower risk of flare-ups.
In comparison to utilising an ICS inhaler alone, combination inhalers allow for the use of lower doses of ICS. With the inclusion of a LABA, it is possible to utilise lower corticosteroid doses while still effectively controlling inflammation, lowering the risk of adverse effects brought on by using greater steroid doses.
5. Long-Acting Bronchodilators
Long-acting bronchodilators (LABAs) play a crucial role in the management of allergic asthma. LABAs produce long-lasting bronchodilation for up to 12 hours, on average. They lessen symptoms including wheezing, shortness of breath, and coughing by keeping the airways open.
In an asthma controller regimen, LABAs are frequently administered in addition to ICS drugs. In order to better manage asthma, this combination of medications helps to reduce both bronchoconstriction and airway inflammation.
Exercise c cause bronchoconstriction in people with allergic asthma. Before engaging in physical activity, LABAs are used to lessen or stop the symptoms that come with exercise.
It's crucial to remember that LABAs must never be administered alone; because it increases the risk of severe asthma exacerbations. In contrast, LABAs must always be combined with ICS. Working closely with a healthcare professional is essential in order to develop an effective treatment plan for allergic asthma, which include the use of LABAs, based on the patient's symptoms, the severity of their asthma, and other variables.
6. Short-Acting Bronchodilators
Short-acting bronchodilators primarily work by relaxing the smooth muscles surrounding the airways. They exert their action on bronchial smooth muscle beta-2 adrenergic receptors, causing relaxation and bronchodilation as a result. This enhances airflow and lessens asthmatic symptoms.
During acute episodes of bronchoconstriction, short-acting bronchodilators offer quick relief, opening the airways and enabling the return of normal breathing. They take effect quickly—often in a matter of minutes—and their effects persist for several hours.
When it comes to treating acute asthma symptoms, short-acting bronchodilators are recommended as the first line of defence. They are frequently prescribed for occasional usage to treat sporadic or mild asthma. When symptoms arise or in response to triggers such as allergen exposure, exercise-induced bronchoconstriction, or respiratory infections, patients are recommended to use them as needed.
Short-acting bronchodilators are often a crucial part of special asthma treatment. These strategies are developed in conjunction with healthcare professionals to help people manage their asthma symptoms and modify their drug regimens in accordance with their specific needs. In action plans for treating acute symptoms, short-acting bronchodilators are frequently suggested as the first line of therapy.
Can the treatment of allergies be used to treat allergic asthma?
Yes, allergic asthma is treated using the same methods used to treat allergies. The main objectives of treating allergic asthma include symptom management and control, lowering the frequency and intensity of asthma attacks, and enhancing the general quality of life for those who have this condition. The treatment strategy frequently combines medicine and methods for avoiding allergens. Here are a few typical asthmatic allergy treatments:
Inhaled corticosteroids(ICS) are the most effective medications for allergic asthma. Inhaled corticosteroids primarily do this function by recruiting the enzyme histone deacetylase 2 (HDAC2) to reverse histone acetylation, which turns off a number of active inflammatory genes.
With the help of reducing inflammatory airway response, ICS alleviate asthma symptoms and lessen airway hyperresponsiveness.ICS are now the first-line treatment option for managing asthma symptoms and avoiding exacerbations for all patients with chronic asthma. Inhaled long-acting 2-agonists are frequently administered in addition to ICS to further improve asthma control, which increases compliance and manages asthma at lower dosages of corticosteroids, In COPD, however, ICS offer substantially less therapeutic benefit, because the inflammation is resistant to corticosteroid impact.
Immunomodulators play an important role in the management of allergic asthma. Immunomodulators are drugs that assist in controlling and modifying the immune system's reaction. Immunomodulators are used to control the heightened immune reaction to allergens in the setting of allergic asthma, thereby lowering inflammation and airway hyperresponsiveness.
Monoclonal antibodies are a more recent family of immunomodulators that target particular immune response-related components. Omalizumab and dupilumab are examples of monoclonal antibodies that are used to treat allergic asthma. Immunoglobulin E (IgE), a factor in allergic reactions, is inhibited by omalizumab. Dupilumab targets interleukin-4 (IL-4) and interleukin-13 (IL-13), which are involved in the allergic inflammatory response.
The long-term management of asthma symptoms is managed with the help of combination asthma inhalers. They mix a corticosteroid and a long-acting beta-agonist (LABA), which are two separate inhaled drugs. LABAs are bronchodilators that widen and open congested airways to allow for the free flow of air, whereas corticosteroids reduce inflammation. These drugs work better together to reduce airway hyperresponsiveness and prevent asthma attacks.
LABA functions by relaxing the smooth muscles that surround the airways, which opens up the airways and enhances airflow. Wheezing and breathlessness are reduced as a result of this. Formoterol and salmeterol are two commonly used LABAs.
Long-acting bronchodilators (LABAs) play a crucial role in the management of allergic asthma. LABAs produce long-lasting bronchodilation for up to 12 hours, on average. They lessen symptoms including wheezing, shortness of breath, and coughing by keeping the airways open.
In an asthma controller regimen, LABAs are frequently administered in addition to ICS drugs. In order to better manage asthma, this combination of medications helps to reduce both bronchoconstriction and airway inflammation.
Short-acting bronchodilators primarily work by relaxing the smooth muscles surrounding the airways. They exert their action on bronchial smooth muscle beta-2 adrenergic receptors, causing relaxation and bronchodilation as a result. This enhances airflow and lessens asthmatic symptoms.
During acute episodes of bronchoconstriction, short-acting bronchodilators offer quick relief, opening the airways and enabling the return of normal breathing. They take effect quickly—often in a matter of minutes—and their effects persist for several hours.
Are the medications for allergic asthma available in an online pharmacy?
Yes, allergy medications are commonly available in online pharmacies. Online pharmacies offer a wide range of medications, including over-the-counter (OTC) and prescription allergy medications. These online platforms provide a convenient way to purchase medications without having to visit a physical pharmacy.
It's also worth noting that the availability of specific allergy medications varies depending on the location and the regulations governing the sale and distribution of medications in the country or region. Always consult with a healthcare professional or pharmacist to determine which allergy medication is suitable for you and whether it can be purchased online.
What are the ways to manage allergic asthma?
Listed below are the methods to manage allergic asthma.
- Prevention
An all-encompassing strategy that involves precautions, medication, and preventive therapies is required for the management of allergic asthma.
- Avoiding triggers
Reducing triggers and preventing asthma episodes depend heavily on patient education, allergen avoidance, and environmental management. Avoiding triggers is the first line of protection for treating allergic asthma. People ought to identify their unique allergens and take precautions to reduce exposure. This includes avoiding environmental triggers like pollen and pollution as well as maintaining clean, mold- and dust-mite-free, pet-free inside surroundings.
- Medications
In order to alleviate symptoms and enhance lung function, doctors frequently prescribe drugs including inhaled corticosteroids, long-acting beta-agonists, leukotriene modifiers, and short-acting beta-agonists. Immunomodulators and combination inhalers could be required for people with severe allergic asthma.
Is allergic asthma dangerous?
Yes, Allergic asthma is a serious condition, and if not properly managed, it is potentially dangerous. The severity of allergic asthma varies from person to person.
Although some people only have moderate symptoms that are managed with medication, others may experience more severe episodes that happen more frequently. A severe asthma attack may be fatal, requiring rapid medical care






 Rated Excellent by 26,523+ Reviews
Rated Excellent by 26,523+ Reviews